Troponin measurement is well-established in the diagnosis of heart attacks, and high-sensitivity cardiac troponin is now the recommended test in the diagnosis of heart attacks (MI/ACS).i But the biomarker has far more uses: with troponin being a sensitive indicator of individual heart health, the risk of heart disease can be estimated in advance.ii Here are 5 facts that you need to know about troponin and the high sensitive troponin I test from Abbott.
1. Knowledge of their risk increases motivation of patients
In a representative survey among 2026 people aged 18 and over conducted by the YouGov polling institute, 83% of the surveyed men and 91% of the women stated that they would change their lives if a test showed an individually increased risk of heart attack1. Such a test can therefore help to motivate patients to implement lifestyle modifications and thus live a long and healthy life.
A heart health indicator can also be a useful tool in therapy monitoring by making the progress of therapy measurable and visible to the patient.
2. Risk stratification in primary prevention benefits doctors and patients
Risk stratification of asymptomatic people, who are otherwise considered healthy, can save time and resources in two ways:
Therefore, there is growing interest and discussion of making the measurement of high-sensitivity cardiac troponin I (hs-cTnI) a permanent part of regular health check-ups in the future.v,vi,vii In this way, the troponin I value as a cardiac specific marker could give additional information about the individual cardiovascular health risk and inform the decision on the management of other clinical findings (e.g. lipids, blood pressure), for example by guiding stricter target values.
3. Not all troponins are the same
Troponins are heart-specific biomarkers; for risk stratification, they are superior to non-specific markers such as the high-sensitivity C-reactive protein (hsCRP). However, not all troponins are equal: troponin I, for example, is significantly less affected by kidney function than troponin T.viii Additionally, Troponin I is not affected by skeletal muscle interference like Troponin T.ix,x In addition, Abbott’s highly sensitive troponin I test is not affected by biotin (vitamin B7 or vitamin H) – a common problem in other laboratory tests because biotin is still increasingly popular as a dietary supplement.xi
4. Different cut-off values apply to men and women
Women usually have lower troponin I levels than men.xii For this reason, a highly sensitive test that can detect even very small amounts of the protein troponin is particularly advantageous for women. Troponin I values of < 6 ng/l (men) and < 4 ng/l (women) indicate a low risk of future heart disease in conjunction with clinical and diagnostic findings. Values above this level may indicate subclinical myocardial damage and an increased risk of future heart disease (fig. 1).xiii In such patients, it is important to find out the cause of the increased troponin I levels and to check which risk factors (e.g. type 2 diabetes and hypertension) have not yet been identified.
In the next step, appropriate treatment should then be initiated or an existing therapy adapted: In accordance with the current guideline recommendations, a healthy lifestyle with sufficient exercise and a balanced diet as well as adequate blood pressure and lipid control is recommended for people with a medium or high cardiovascular risk, if necessary by means of pharmacotherapeutic interventions.xiv The aim of these measures is to reduce cardiovascular risk and prevent cardiac diseases such as myocardial infarction and heart failure.
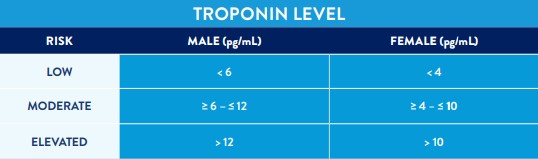 |
Figure 1: Cut-off values for troponin I in men and women without manifest heart disease, and resulting interpretation (cut-off values derived from xv,xvi,xvii,xviii).
5. No consensus regarding the ideal time for the initial risk assessment
To date, there is neither a recommendation from the major cardiological societies nor a consensus among experts as to when risk stratification using the Troponin I test should be offered for the first time. Professor Dr. Christoph Liebetrau from the Heart Centre in Bad Nauheim, Germany, considers an examination of cardiovascular health to be useful for men aged 50 and over and for women aged 60 and over. Dr. Winfried März, Professor of Medical and Chemical Laboratory Diagnostics at the Medical University of Graz (Austria) and Director of the SYNLAB Academy in Germany, takes a similar view. He recommends troponin measurement for men aged 50 and over and for women aged 55 and over. However, even in younger years it can be useful to determine troponin in order to assess the personal, individual risk.
The guidelines of the European Society of Cardiology (ESC) and the German Society of Cardiology (DGK) published in 2016 recommend systematic assessment of total cardiovascular risk using a risk estimation system such as SCORE (Systematic Coronary Risk Estimation) in individuals at increased risk, i.e. those with a family history of premature cardiovascular disease, familial hyperlipidemia, major cardiovascular risk factors (such as smoking, high blood pressure, diabetes mellitus or raised lipid levels) or comorbidities increasing cardiovascular risk.xix In addition, systematic CV risk assessment may be considered in men > 40 years of age and in women > 50 years of age or post-menopausal with no known cardiovascular risk factors.
 |
More about Abbott‘s high sensitivity troponin I test
Abbott's highly sensitive troponin I test is the first and only troponin test to receive the CE mark for being used, in conjunction with clinical and diagnostic findings, to aid in stratifying the risk of cardiovascular disease in asymptomatic individuals.
References
i Thygesen K, Alpert JS, Jaffe AS et al. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019; 40(3):237-269.
ii Jia X, Sun W, Hoogeveen RC et al. High-Sensitivity Troponin I and Incident Coronary Events, Stroke, Heart Failure Hospitalization, and Mortality in the ARIC Study. Circulation. 2019; 139(23):2642-2653.
iii Blankenberg S, Salomaa V, Makarova N et al. Troponin I and cardiovascular risk prediction in the general population: the BiomarCaRE consortium. Eur Heart J. 2016; 37(30):2428-37.
iv Diederichs C, Neuhauser H, Rücker V et al. Predicted 10-year risk of cardiovascular mortality in the 40 to 69 year old general population without cardiovascular diseases in Germany. PLoS One. 2018; 13(1):e0190441.
v Omland T, de Lemos JA, Holmen OL et al. Impact of sex on the prognostic value of high-sensitivity cardiac troponin I in the general population: the HUNT study. Clin Chem. 2015; 61(4):646-56.
vi Sigurdardottir FD, Lyngbakken MN, Holmen OL et al. Relative Prognostic Value of Cardiac Troponin I and C-Reactive Protein in the General Population (from the Nord-Trøndelag Health [HUNT] Study). Am J Cardiol. 2018; 121(8):949-955.
vii Ford I, Shah AS, Zhang R et al. High-Sensitivity Cardiac Troponin, Statin Therapy, and Risk of Coronary Heart Disease. J Am Coll Cardiol. 2016; 68(25):2719-2728.
viii Freda BJ, Tang WH, Van Lente F et al. Cardiac troponins in renal insufficiency: review and clinical implications. J Am Coll Cardiol. 2002; 40(12):2065-71.
ix Jaffe AS, Vasile VC, Milone M, et al. Diseased skeletal muscle: A noncardiac source of increased circulating concentrations of cardiac troponin T. J Am Coll Cardiol 2011; 58:1819-1824.
x Rittoo D, Jones A, Lecky B, Neithercut D. Elevation of cardiac troponin T, but not cardiac troponin I, in patients with neuromuscular diseases: Implications for the diagnosis of myocardial infarction. J Am Coll Cardiol 2014; 63:2411-2420.
xi Frame IJ, Joshi PH, Mwangi C et al. Susceptibility of Cardiac Troponin Assays to Biotin Interference. Am J Clin Pathol. 2019; 151(5):486-493.
xii Shah AS, Griffiths M, Lee KK et al. High sensitivity cardiac troponin and the under-diagnosis of myocardial infarction in women: prospective cohort study. BMJ. 2015; 350:g7873.
xiii Everett BM, Zeller T, Glynn RJ et al. High-sensitivity cardiac troponin I and B-type natriuretic Peptide as predictors of vascular events in primary prevention: impact of statin therapy. Circulation. 2015; 131(21):1851-1860.
xiv Piepoli MF, Hoes AW, Agewall S et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2016; 37(29):2315-2381.
xv Zeller T, Tunstall-Pedoe H, Saarela O et al. MORGAM Investigators. High population prevalence of cardiac troponin I measured by a high-sensitivity assay and cardiovascular risk estimation: the MORGAM Biomarker Project Scottish Cohort. Eur Heart J. 2014; 35(5):271-281.
xvi Omland T, Pfeffer M, Solomon S et al. For the PEACE Investigators. JACC Vol. 61, No. 12, 2013 Omland et al. 1241 March 26, 2013:1240–1249 Troponin I in Stable CAD.
xvii Cavender MA, White WB, Jarolim P, et al. Serial Measurement of High-Sensitivity Troponin I and Cardiovascular Outcomes in Patients With Type 2 Diabetes Mellitus in the EXAMINE Trial (Examination of Cardiovascular Outcomes With Alogliptin VersusStandard of Care). J Am Heart Assoc. 2017, 135:1911-1921.
xviii Eisen A, Bonaca MP, Jarolim P, et al. Clinical Chemistry 63:1 307-315 (2017) Lipids, Lipoproteins, and Cardiovascular Risk Factors.
xix Hambrecht R, Albus C, Halle M. Prävention von Herz-Kreislauf-Erkrankungen. Börm Bruckmeister Verlag 2016.
Links, die Sie von den weltweiten Abbott-Websites zu anderen Seiten leiten, unterliegen nicht der Kontrolle durch Abbott und Abbott ist nicht für die Inhalte einer solchen Website oder untergeordnete Links solcher Websites verantwortlich. Abbott stellt diese Links nur als weiterführende Informationen zur Verfügung, und die Einbeziehung eines Links bedeutet nicht, dass Abbott die verlinkte Seite billigt.
Die Website, die Sie angefordert haben, ist vielleicht nicht für Ihre Bildschirmgröße optimiert.